

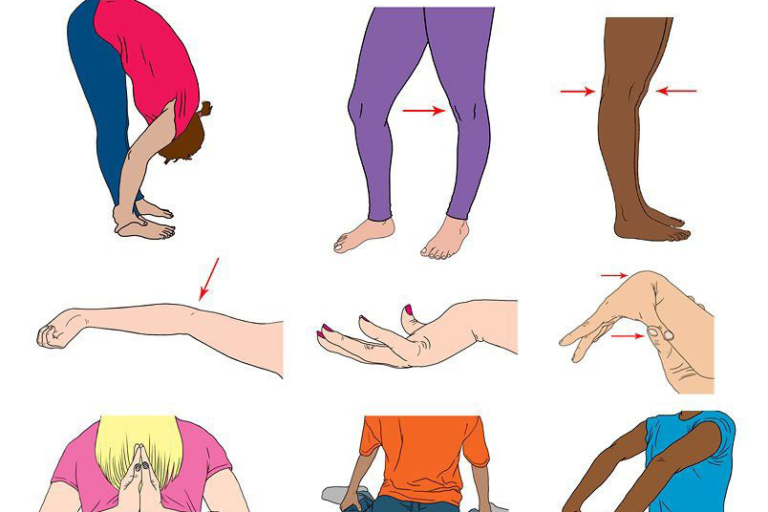
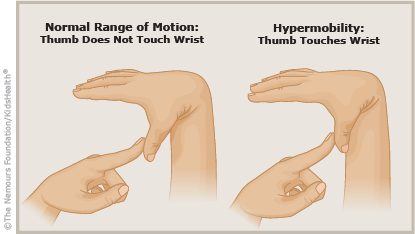
Have you ever met someone who could touch their thumb to their forearm or drop into the splits without warm-up? While it might look impressive, these party tricks could signal more than flexibility: they might be signs of a medical condition called hypermobility syndrome.
What Is Hypermobility Syndrome?
Joint hypermobility simply means that a person’s joints move beyond the normal range expected for a particular joint. For many, this is harmless. However, when this flexibility may come with symptoms like pain, fatigue, joint instability, or frequent injuries, it may be diagnosed as hypermobility spectrum disorder (HSD) or hypermobile Ehlers-Danlos syndrome (hEDS): two recognised conditions on the hypermobility spectrum.
Hypermobility syndrome affects a wide range of people: dancers, gymnasts, children, and even office workers, often going undiagnosed for years. A growing body of research is now helping clinicians to better understand and manage the condition.
The Evolution of the Diagnosis: HSD vs hEDS
In 2017, the classification of hypermobility-related conditions was revised by the International Consortium on the Ehlers-Danlos Syndromes. Previously grouped under “Joint Hypermobility Syndrome” (JHS), the condition was separated into:
- Hypermobility Spectrum Disorder (HSD) – for those with symptoms but who do not meet the strict criteria for a connective tissue disorder.
- Hypermobile Ehlers-Danlos Syndrome (hEDS) – a hereditary disorder of connective tissue, often more severe, requiring more rigorous diagnostic criteria.
This separation helps tailor treatment plans and allows for a more accurate prognosis and support.
Diagnosing hEDS or HSD requires:
- A detailed medical and family history
- Assessment of systemic features (e.g., skin, gastrointestinal, cardiovascular involvement)
- Clinical scoring systems like the Beighton Score (assessing joint laxity)
- Exclusion of other connective tissue disorders
🔍 Example: A 28-year-old female yoga instructor presents with knee pain, shoulder subluxations, and chronic fatigue. Her Beighton Score is 6/9, she reports easy bruising and gastrointestinal discomfort, but no family history. After excluding other disorders, she is diagnosed with hypermobility spectrum disorder and referred for physiotherapy and symptom management.
Common Symptoms of Hypermobility Syndrome
Hypermobility syndrome isn’t just about flexible joints: the symptoms can be broad and life-affecting. Common complaints include:
-
Chronic joint pain or fatigue
-
Joint instability or frequent dislocations
-
Poor proprioception (reduced body awareness)
-
Gastrointestinal issues (e.g., IBS-like symptoms)
-
Postural Orthostatic Tachycardia Syndrome (POTS)
-
Anxiety or mood disorders
Soft, stretchy skin or delayed wound healing
Why Early Diagnosis Matters
Early diagnosis allows individuals to receive tailored care, prevent injury, and avoid inappropriate treatments. Misdiagnosis is common: many people are incorrectly treated for fibromyalgia, chronic fatigue syndrome, or psychosomatic disorders.
🧠 Did You Know? Research by Tinkle et al. (2017) suggests that up to 80% of people with hEDS experience autonomic dysfunction, contributing to dizziness, fatigue, and digestive issues.
Managing Hypermobility Syndrome: A Multidisciplinary Approach
There is currently no cure for hypermobility disorders, but symptoms can be managed effectively through a combination of therapies. Key pillars of treatment include:
1. Physiotherapy: The Cornerstone of Care
At Destiny Health, we see first-hand how individualised exercise programs can improve function and reduce pain. Physios focus on:
-
Stabilisation exercises for major joints (especially hips, shoulders, knees)
-
Motor control and proprioception training
-
Pacing strategies to manage fatigue
- Education on joint protection techniques🧍 Example: A 15-year-old male with shoulder dislocations from playing basketball attends physiotherapy. Over 3 months, he progresses from banded isometric work to resisted shoulder stabilisation and core training, significantly reducing his dislocations.
🧍 Example: A 15-year-old male with shoulder dislocations from playing basketball attends physiotherapy. Over 3 months, he progresses from banded isometric work to resisted shoulder stabilisation and core training, significantly reducing his dislocations.
2. Occupational Therapy
OTs assist with daily adaptations for energy conservation and joint protection in tasks like dressing, driving, and computer work.
Tools might include:
- Ergonomic chairs
- Splints or braces for hypermobile fingers
- Voice recognition software to reduce typing load
3. Pain Management
Chronic pain is common and often needs a multi-modal approach:
- Low-impact aerobic exercise (e.g., swimming, Pilates)
- Cognitive Behavioural Therapy (CBT) for pain perception
- Low-dose tricyclic antidepressants or SNRIs under medical supervision
Topical NSAIDs over oral options (to reduce GI side effects)
4. Lifestyle & Nutrition
Emerging evidence suggests that anti-inflammatory diets may help reduce systemic symptoms. While more research is needed, many patients report improvements when reducing processed foods, sugar, and dairy.
Hydration, magnesium supplementation, and collagen support (e.g., glycine-rich foods) may benefit connective tissue, though individual response varies.
5. Addressing Comorbidities
Many people with hypermobility syndrome experience overlapping conditions. Managing these is essential for holistic care:
-
POTS: Managed through salt/fluid intake, compression garments, and graded exercise
-
Anxiety: Seen in up to 70% of hEDS individuals (Bulbena et al., 2011), CBT is a frontline treatment
- Gastrointestinal Issues: Often managed with dietitian support and gut-directed therapies
What About Children and Adolescents?
Children with hypermobility often appear “clumsy” or complain of “growing pains.” Many outgrow excessive flexibility as joints stiffen with age, but others continue to experience symptoms into adulthood.
🔄 A tailored play-based exercise program, combined with parental education and school support, often helps children thrive without reinforcing fear or avoidance behaviours.
Exercise: Friend or Foe?
Yes, hypermobile individuals should exercise: but wisely.
Key recommendations:
- Avoid end-range stretching or ballistic movements
- Emphasise slow, controlled strength training
- Build core stability and joint alignment
- Start with short sessions and gradually build tolerance
💡 At Destiny Health, we often use reformer Pilates and closed-chain bodyweight exercises like wall sits or glute bridges to activate key muscle groups without joint overload.
The Role of Mental Health
Many people with hypermobility syndrome experience anxiety, depression, and sometimes even health anxiety. The unpredictability of symptoms, frequent medical visits, and chronic fatigue can contribute significantly to distress.
Psychological support, whether via a psychologist or support group, is often essential. A 2020 systematic review (Smith et al.) noted that acceptance-based therapies were particularly effective in chronic hypermobility-related pain.
Latest Research & Emerging Insights
- Connective Tissue Genetics: Ongoing genetic studies are identifying variants associated with hEDS, though no single gene is yet confirmed (Malfait et al., 2017).
- Fascia Dysfunction: Some researchers propose that fascial dysfunction plays a larger role in hypermobility-related pain than previously thought.
- Gut-Joint Axis: There’s growing interest in the relationship between connective tissue and the microbiome, especially in patients with IBS-like symptoms.
These insights could lead to more targeted therapies in the next decade.
When to Seek Help
You should consult a healthcare provider if you or your child experience:
- Frequent joint dislocations or sprains
- Unexplained fatigue or dizziness
- Recurrent gastrointestinal issues
- Generalised joint pain not improving with rest
Destiny Health offers thorough assessment, patient-centred physiotherapy, and referral pathways for further diagnosis when needed.
Final Thoughts
Hypermobility syndrome is more than just being “double-jointed,” it’s a complex condition that, when understood and managed properly, allows individuals to live full, active lives. With early intervention, education, and a tailored exercise plan, symptoms can be controlled, and quality of life significantly improved.
References
- Tinkle, B. T., et al. (2017). Hypermobile Ehlers-Danlos Syndrome (hEDS). American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 175(1), 48–69. https://doi.org/10.1002/ajmg.c.31538
- Malfait, F., Francomano, C., Byers, P., et al. (2017). The 2017 international classification of the Ehlers–Danlos syndromes. American Journal of Medical Genetics Part C, 175(1), 8–26. https://doi.org/10.1002/ajmg.c.31552
- Bulbena, A., et al. (2011). Anxiety disorders in the joint hypermobility syndrome. Psychiatry Research, 197(1–2), 56–60. https://doi.org/10.1016/j.psychres.2011.01.015
- Smith, T. O., et al. (2020). Interventions for people with joint hypermobility syndrome and hypermobile Ehlers–Danlos syndrome: A systematic review. Rheumatology Advances in Practice, 4(2), rkaa031. https://doi.org/10.1093/rap/rkaa031
- Castori, M., et al. (2012). Chronic fatigue syndrome and joint hypermobility syndrome: Two overlapping conditions? Clinical and Experimental Rheumatology, 30(2), 191–196.
- Celletti, C., et al. (2021). Rehabilitation of joint hypermobility syndrome/hEDS: A consensus statement of the EDS International Consortium. Frontiers in Rehabilitation Sciences, 2. https://doi.org/10.3389/fresc.2021.722834