

Anterior Cruciate Ligament (ACL) injuries are among the most common and devastating in sport. Whether you’re an elite athlete or a weekend warrior, a torn ACL can feel like a crushing blow. But with the right surgical approach and a structured rehabilitation plan, a strong and confident return to sport is absolutely possible.
At Destiny Health, we’ve combined the latest research from world-class clinicians and academics like Mick Hughes, Randall Cooper, Claire Ardern, and others to bring you an evidence-informed guide to navigating every stage of ACL reconstruction rehab.
Contents
- Understanding the ACL and Its Role
- Surgical Options: Graft Types and Trends
- Return: A Guide to ACL Reconstruction RehabPost-Operative Challenges You Should Know
- The Five Stages of ACL Rehabilitation
- Return to Sport: Criterion-Based, Not Time-Based
- Psychological Readiness: The Forgotten Factor
- Final Thoughts
- References
1. Understanding the ACL and Its Role
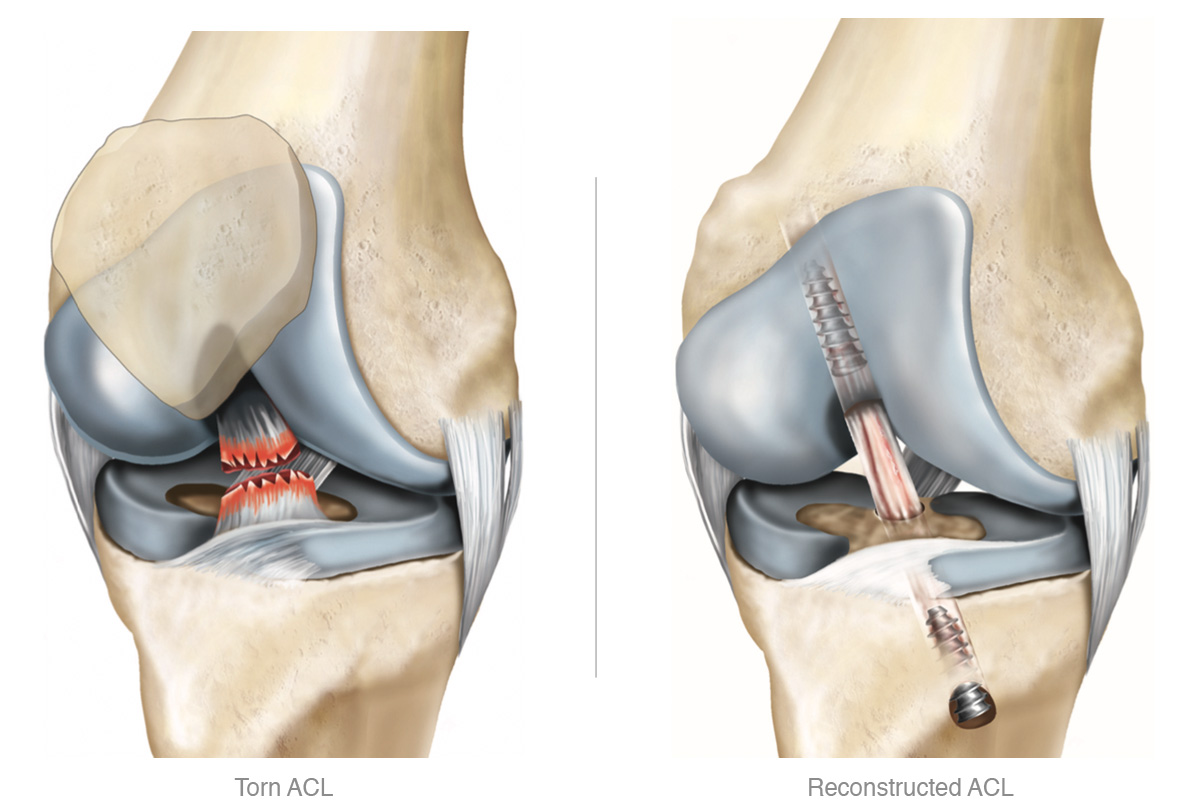
The ACL is one of the key stabilising ligaments in the knee. It prevents anterior (forward) translation of the tibia and provides rotational stability. ACL ruptures typically occur during non-contact movements such as cutting, pivoting, or landing awkwardly.
Tears do not always require surgery. However, for young, active individuals wanting to return to high-level pivoting sports, ACL reconstruction (ACLR) is generally recommended.

2. Surgical Options: Graft Types and Trends
ACL reconstruction involves replacing the torn ligament with a graft. The most common types include:
Hamstring Tendon Autograft (from the patient’s own lower limb): Popular due to low donor-site morbidity (illness), but may result in hamstring weakness.
Bone-Patellar Tendon-Bone (BPTB) Autograft: Favoured for its high tensile strength and faster bone integration, often used in high-level athletes.
Quadriceps Tendon Autograft: Growing in popularity, particularly for its favourable size and strength.
Allografts (from cadavers (deceased)): Typically used in older or less active populations due to slower integration and higher failure rates.
Surgeons often tailor their choice based on sport, age, sex, and patient preference.
3. Post-Operative Challenges You Should Know
Rehab isn’t always smooth sailing. Some common issues include:
- Knee Stiffness and Arthrofibrosis: Especially if early range of motion is neglected.
- Graft Failure: Often due to premature return to sport or poor rehab compliance.
- Muscle Atrophy: Quadriceps inhibition is common and can delay progression.
- Patellofemoral Pain: Particularly after BPTB grafts.
- Psychological Barriers: Fear of re-injury can be just as limiting as physical factors.
4. The Five Stages of ACL Rehabilitation
The Melbourne ACL Rehabilitation Guide 2.0, developed by Mick Hughes and Randall Cooper, outlines a progressive, criterion-based model across five phases:
Phase 1: Acute Phase (0–4 weeks)
Goals:
- Reduce pain and swelling
- Achieve full passive extension and 90°+ flexion
- Restore quadriceps activation and normal gait
Key Interventions:
- Ice, compression, elevation
- Heel slides, quad sets, patella mobilisation
- Stationary bike, supported gait retraining
Common Mistake: Overprotecting the knee: early mobilisation is essential.
Phase 2: Strength & Neuromuscular Control (4–12 weeks)
Goals:
- Restore full ROM
- Begin progressive strengthening
- Regain neuromuscular control
Exercises:
- Bodyweight squats, step-ups, bridges
- Resistance band work
- Balance training and proprioception
Milestone: Symmetrical range of motion and minimal swelling.
Phase 3: Running and Agility (12–20 weeks)
Goals:
- Achieve baseline strength (70%+ limb symmetry index)
- Begin linear running and low-level agility drills
Tests:
- Single-leg squats
- Y-Balance Test
- Hop preparation drills
Key Point: Avoid reintroducing pivoting sports too early.
Phase 4: Return to Sport (5–9 months)
Goals:
- 90%+ strength symmetry
- High-level agility and plyometrics
- Reintroduce sport-specific movements
Assessment Tools:
- Triple hop test
- Isokinetic strength testing
- Psychological readiness scales (e.g. ACL-RSI)
Warning: Time alone is not a reliable indicator of readiness.
Phase 5: Return to Performance (9–18 months)
Goals:
- Match or exceed pre-injury performance
- Reduce reinjury risk
- Load tolerance in full competition
Strategies:
- Continue neuromuscular training
- Fatigue-based sport simulation drills
- Biomechanical feedback and video analysis
Gold Standard: Full confidence and symmetrical power output on all tests.
5. Return to Sport: Criterion-Based, Not Time-Based
Claire Ardern and colleagues have shown that simply waiting six or nine months isn’t enough. Athletes should meet specific criteria across physical and psychological domains:
Return to Sport Criteria:
- ≥ 90% limb symmetry on hop tests
- ≥ 90% quadriceps and hamstring strength
- No pain or swelling
- Completion of sport-specific drills
- Psychological readiness (high ACL-RSI score)
Failing to meet these significantly increases reinjury risk.
6. Psychological Readiness: The Forgotten Factor
Fear of reinjury, lack of confidence, and reduced motivation can all derail rehab. Psychological readiness is now considered one of the most powerful predictors of successful return to sport.
Tips to Improve Confidence:
- Gradual exposure to sport-specific drills
- Use of video feedback
- Regular check-ins with your physio or coach
- Incorporation of mental skills training (visualisation, self-talk)
Tools like the ACL-RSI scale can help track progress and flag concerns early.
7. Final Thoughts
ACL rehab isn’t just a physical process, it’s a journey of mindset, movement, and milestones.
By understanding the surgical options, managing common setbacks, and progressing through a structured, evidence-informed rehab plan, clients can set themselves up for the best possible outcome.
Remember: time doesn’t heal – smart rehab does.
At Destiny Health, we’re here to support you every step, jump, and sprint along the way.
References
- Ardern, C. L., Taylor, N. F., Feller, J. A., & Webster, K. E. (2018). Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. British Journal of Sports Medicine, 52(2), 128–138.
- Cooper, R., & Hughes, M. (2020). Melbourne ACL Rehabilitation Guide 2.0. [Online]. Available at: https://www.ricmellor.com/melbourne-acl-guide
- Grindem, H., et al. (2016). Return to sport after ACL reconstruction: association with second ACL injury and patient-reported outcomes. British Journal of Sports Medicine, 50(9), 746–753.
- Hughes, M., & Cooper, R. (2022). Evidence-Based ACL Rehab Progressions. Sports Physio Journal, 34(1), 21–30.
- Webster, K. E., Feller, J. A., & Ardern, C. L. (2020). Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British Journal of Sports Medicine, 54(7), 356–363.
- Gokeler, A., et al. (2019). The return to sport after ACL reconstruction: a decision-making algorithm integrating load progression and psychological readiness. International Journal of Sports Physical Therapy, 14(3), 465–478.
- Dingenen, B., & Gokeler, A. (2020). Optimization of the return-to-sport paradigm after ACL injury: a critical step back to move forward. Sports Medicine, 50(5), 725–730.